March 13, 2012
Cows are amongst the gentlest of breathing creatures; none show more passionate tenderness to their young when deprived of them; and, in short, I am not ashamed to profess a deep love for these quiet creatures.
Thomas de Quincey (1785-1859), Confessions of an English Opium-Eater (1822-1856)
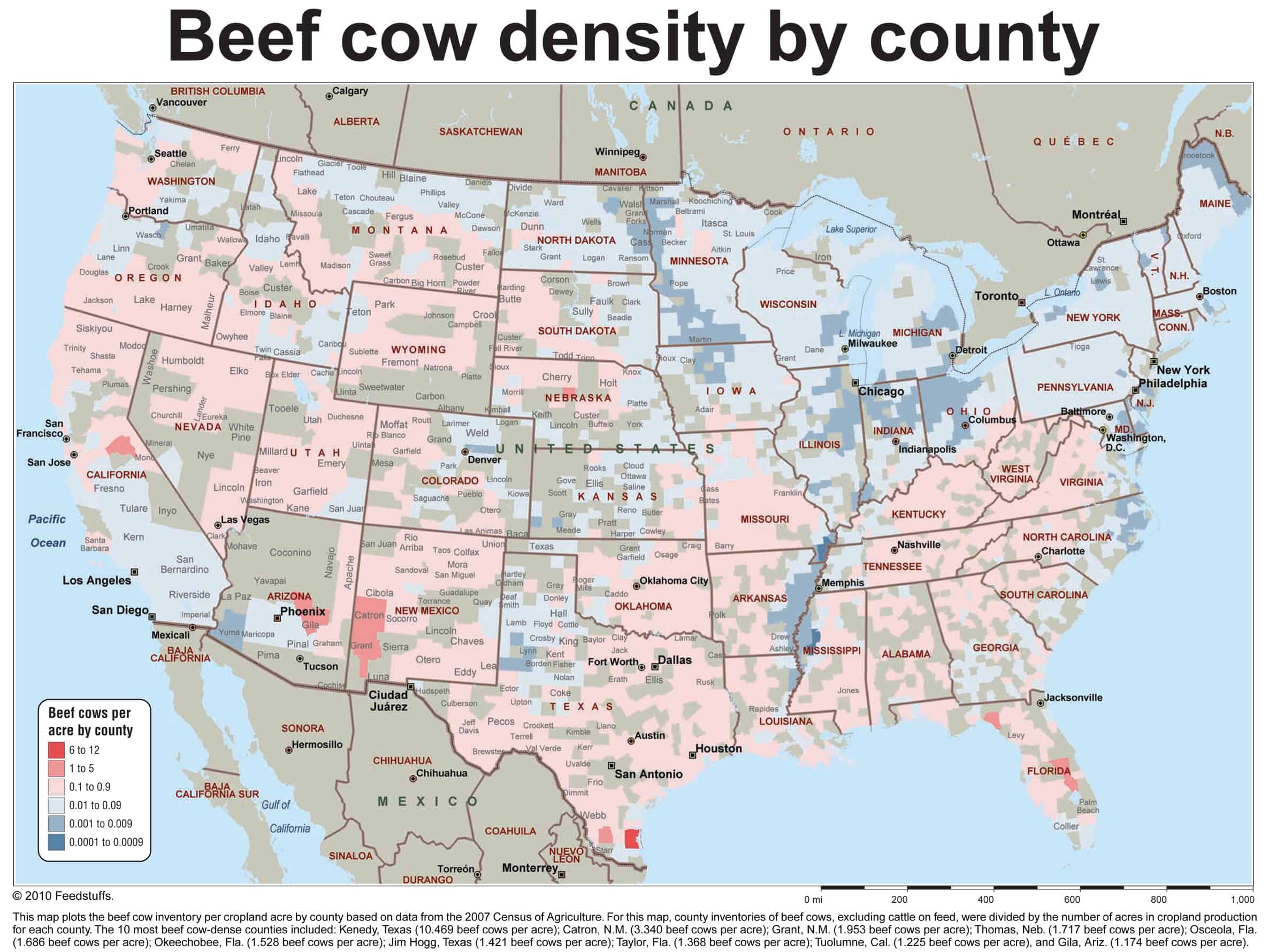
At a recent healthcare innovations summit, Atul Gawande used the United States robust data-driven agricultural industry as a model that healthcare should emulate and commented that we even know the number of cows in every county. It is hard to imagine how cows have anything to do with healthcare-acquired infections. The former are gentle creatures that mankind has benefited from for ages, and the latter is an unrelenting plague causing significant death and disability in untold numbers. It is estimated that these infections affect one-in-twenty hospitalized patients, but besides estimates and projections, there is little hard evidence, just scant data from handpicked references or reports in the literature.
However, having data on the strength of the enemy is essential in any armed engagement and the question must be asked, if we have a map that shows the number of cows in each county in America, why don t we have a map that shows the rates of deadly superbugs such as MRSA or for that matter all of the major bacteria that cause healthcare-acquired infections (HAIs)?
We are not experts in agriculture, and thus, cannot know the complexities of ranching. However, we have seen what is going on in medicine and can only guess what may have taken place in generating the data for the cow density map.
If medicine were run like agriculture we would have a map for MRSA, but if agriculture were run like medicine the following may have taken place in the derivation of the cow map. Please indulge in the following absurdity:
First, there was intense disagreement on what a cow is. Not everyone used the same definition. Some farmers defined cows as black-haired mammals with at least four white spots, while others defined them as four-legged mammals with three black spots. Confusion certainly prevailed. Some farmers asked whether cows in ponds are counted the same as cows eating grass. It was then decided to only count cows standing in streams. Called Cow Stream Infestations (CSIs) or cowteremia, this classification provided data that some praised and all could agree upon. But the CSIs occurred so infrequently that a meaningful comparison between farms could not be made.
And who was going to pay for the farmhands to count the cows? After all, counting them would not change the number of cows on the farm and it was ultimately viewed as wasted effort. In addition, the time that farmhands spent counting could be used to do other things.
So as not to burden the farm, initially counting was done on the basis of farm income tax returns showing the number of cows sold. But only about half of the cows were tabulated because of software limitations. It was then decided to have the farmhands count the cows in the field.
Because of the difficulties in counting individual cows, some states thought it would be easier to just count cow herds. However, no one could agree on how many cows constituted a herd. A definition that was finally agreed upon was that a herd was a group of cows that was more than the usual number on a farm. No one could agree on what a usual number was and thus few herds or cows were actually reported.
One state counted two cow herds that year; a true landmark for cow counting! Other states reported no cow herds whatsoever. It was later found that many cows were not counted that first year due to a low number of farmhands, as scores were fired because of financial cutbacks. In addition, no one was verifying if the counting was being done properly.
Of course, farms with less than 25 acres weren’t required to count cows, as their cow population was deemed negligible.
Another problem was the cows drifting onto farms from other counties. Fences were proposed to prevent this. But these were deemed too expensive. The great fence conspiracy then started. Two farms were found that had put up poor fences. One of these farms was not even in the United States. These two examples were used to argue that fences did not always work, and thus, no conclusions or recommendations for intervention could be made to address the wandering cow problem.
After years of discussion, meetings, research, and legal action, it occurred to a few farmers that counting was important. It became clear that counting cows was vital to the financial success of farms, overall cow health, fence maintenance, and ordering the correct amount of feed and supplies. The cow map was finally able to be made.
————–
If you are a farmer or rancher and have just read our satire, you may be highly incensed by the comparison. We must first say that we have no beef with farmers, and much like Thomas de Quincey, we share a deep love for cows. However, the allegory is an example of how fact is stranger than fiction.
We have chosen the art of satire and metaphor to dissipate the unnecessary obfuscation of healthcare-acquired infections and to bring an ease of understanding to the devastating issue of these infections.
Healthcare acquired infections are a complex problem, made more so by powerful health industry lobbying groups compelling legislatures against reporting and transparency for unconvincing reasons such as problems with definitions and excuses of burdens on hospital personnel.
After all, every one of us will end up utilizing the healthcare system, and as it sadly stands, there are about 1.7 million infections and 100,000 deaths each year attributed to HAIs. It is an epidemic that is now listed by the Agency for Healthcare Research and Quality as one of the top ten causes of death in the United States.
The 2007 beef cow density map is 100% authentic, as the United States Department of Agriculture Census of Agriculture collects data on all farmers and ranchers every five years. Participation in the Census is required by law. The map displays beef cow inventory per cropland acre by county across all counties in the United States. No such system exists in healthcare facilities for the reporting of HAIs. It is this absurdity that bound us to act the knowledge that our farmers are required to report on the number of cows they have while the vast majority of our hospitals, the places we trust with our lives, do not report when a patient leaves worse off because of a methicillin-resistant Staphylococcus aureus (MRSA) hospital-acquired infection.
To clarify our above satire, cows represent HAIs, farmhands represent nurses, fences represent surveillance and farms represent hospitals. Our satire raises a number of issues, including the question of definitions. Surprisingly, the lack of agreement on what constitutes an infection has been a major arguing point against reporting. However, if we do not have standards for reporting, this also means that standards are not present for patient billing and even more importantly for patient treatment. Does this mean a patient with an infection would be correctly diagnosed and treated in one hospital but not another? Though there is some complexity surrounding what constitutes a healthcare-acquired infection, definitions should be devised in a short period of time and not take years to resolve.
The reporting burden has also been used as an excuse not to report. This has caused some states such as Kentucky to only require the reporting of outbreaks (herds in the above example). Kentucky uses the Centers for Disease Control and Prevention definition of an outbreak, which is a frequency of infection above a baseline. However, the definition of a baseline is left up to the facility. Preliminary data from the Kentucky State Department of Public Health revealed only two reports of infection outbreaks by all Kentucky hospitals during 2011. This data validates how grossly under-reported this epidemic really is.
In the case of MRSA, new federal reporting mandates only require MRSA bacteremia cowteremia (CSIs) to be reported among acute care hospitals. At least one study in England has found that MRSA bacteremia occurs too infrequently to allow meaningful comparisons between facilities. Also, once MRSA infections have spread beyond a tissue infection into the bloodstream, the likelihood of survival decreases. Though a fair attempt at a good start, the new federal MRSA reporting mandate is no better than counting Cow Stream Infestations or cowteremia.
Many facilities complain that the requirements to enter reports using the National Healthcare Safety Network are too burdensome and resource-intensive. The use of billing data to capture certain types of infections is less burdensome but has been hampered because CMS is only able to capture the first 9 of 25 diagnostic codes submitted by older billing programs. This has been corrected with newer billing software.
Additionally, small critical access hospitals (rural hospitals with 25 or fewer beds) are not currently required to report. However, these hospitals can also have significant infection rates and because of their size may not have the resources or expertise to deal with them. Reporting should be viewed as a top priority for all healthcare facilities, regardless of size.
Verification of any reported data is also needed. Colorado and California have reporting systems whose data has been brought into question when a 2012 United States Office of Inspector General report found that only about one-in-seven medical errors are reported to the facility s administration.
Surveillance (fences) including detection and isolation has been used for decades for the control of epidemics. However, with HAIs a number of facilities and academicians have fought vigorously against guidelines that incorporate surveillance. Recently, two studies were published in major medical journals that had serious design flaws (fencing problems). We believe these two studies were unreasonably weighted in policy decision making, as there are many other studies showing that active detection and isolation or eradication of MRSA does indeed reduce MRSA infections. The important question is if there are other protocols that have an equal or greater effect in preventing MRSA that do not use surveillance. Prioritization of prevention protocols to serve as guidelines to prevent HAIs is desperately needed. Donald Berwick, co-founder of the Institute for Healthcare Improvement, warned of the stagnation of progress in infection control due to strict adherence of the ethical principle Primum non nocere (first, do no harm), or as Berwick says, is most commonly understand as don t change the status quo unless you re sure. Berwick has offered a guiding principle that is apropos to the debate surrounding active detection and isolation: primum, don’t just stand there.
Finally, one of the major problems that contributes to increased rates of HAIs is too few nurses (farmhands) on staff. The quality and amount of nursing staff have been shown in repeated studies to affect the occurrence of hospital-acquired conditions, infections, and mortality.
We believe our vision of cow counting utopia, applied to HAIs, can contribute to reducing unnecessary and mostly preventable infections and deaths. This satire is not about public reporting, for that introduces another plethora of excuses of why it cannot be done. The satire is about having the data for action, for community and federal response to a large and dangerous epidemic in our nation.
The juxtaposition of the absence of HAI county-level maps in the presence of a cow map is wholly absurd. This is, however, not strictly a medical issue, rather a medical-political (medi-litical ) issue, and as Napoleon Bonaparte reminds us, In politics, an absurdity is not a handicap.
About the Authors:
Dr. Daniel M. Saman, DrPH, MPH, CPH, is a senior epidemiologist at Health Watch USA.
Dr. Kevin T. Kavanagh, MD, MS, is a non-practicing otolaryngologist in Somerset, KY, and founder of Health Watch USA, a 501(c)3 organization whose mission is to promote healthcare transparency and patient advocacy.
Corresponding Author: Kevin Kavanagh, E-Mail: [email protected]
Image credit: Flickr: mattbatt0